








. Note the wire braiding in the delivery sheath (arrow).")


 with further constraint visible across the sphincter of Oddi (arrowhead). There was limited drainage of contrast.")








.")
.")
 shows a tight stricture of the gastric body (arrow).")




.")
.")

.")
 with immediate full expansion.")

 are obscured by contrast.")
Categorised under:
Interventional Radiology
>
Gastrointestinal
>
Stents
Interventional Radiology
>
Hepatobiliary
>
Stents (non covered)
Interventional Radiology
>
Hepatobiliary
>
Stents (covered)
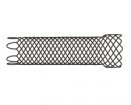
The Korean Egis stents are nitinol stents, with the stent skeleton not woven in a continuous fashion, but "knitted" similar to wire fences. This results in increased flexibility and better conformation to flexures as the stent does not try to regain its straight configuration.
The Korean Egis stents are nitinol stents, with the stent skeleton not woven in a continuous fashion, but “knitted” similar to wire fences. This results in increased flexibility and better conformation to flexures as the stent does not try to regain its straight configuration (Fig 1). Due to the great pliability of the stents they seem to have a natural resistance to migration. In addition the amount of shortening on release is much reduced compared to woven stents (Fig. 2).
Stents are available with a single and a double layer of wire, with and without a covering membrane. The double stents are woven from a thinner gauge nitinol wire, but have the advantage of sandwiching the membrane between the two layers of wire.
As there is a wire mesh on the outside, it allows the stent to be gripped by the mucosa, further reducing the risk of stent migration. The double layers also result in a smaller size of the interstices, claimed to reduce ingrowth into uncovered stents.
The delivery systems have excellent trackability due to nitinol reinforcement (Fig. 3). Enteral systems are only 10Fr. whereas biliary delivery systems are 8Fr. Note that indications for using covered biliary stents are very limited due to the risk of occluding the cystic and other segmental ducts.
As with all nitinol stents radial force increases over time with warming up to body temperature. Initial expansion is often limited with slow increased dilatation over 2-3 days. The pyloric / duodenal stents are identical to the colonic versions except for differing lengths of the delivery systems to accommodate the endoscopy requirements for different scopes. Shortest enteral length for fluoroscopic placement is 80cm. Percutaneous biliary systems are only 50cm long, giving great control over stent position and release.
Although not licensed for use in the oesophagus, we had excellent results with placing 24mm double covered colonic stents in two patients with tracheo-oesophageal fistulae. This was done on a named-patient basis. The large diameter and straight shape resulted in excellent apposition of the whole stent against the oesophageal wall with occlusion of the fistula in both cases. Migration did not occur. A dedicated oesophageal version is awaiting CE marking at the end of January 2011.
The list price is comparable with competitors but discounts are given for high volume users.
Benefits:
Disadvantages:
Transhepatic Insertion of biliary Egis Stent (Double Bare)
A 65-year-old patient with a history of gastric carcinoma presented with obstructive jaundice. The patient previously had a Billroth 2 resection with gastrojejunostomy. CT showed compression of the lower bile duct by a 4cm nodal mass.
A right sided PTC was performed. Injection of contrast through a percutaneous catheter demonstrates a long occlusion of the distal common bile duct with marked dilatation of the proximal biliary tree and a normal distal CBD (Fig. 4). A 10 x 100 mm double bare Egis stent was deployed within the lower end in the duodenum resulting in limited immediate expansion (Fig. 5). Balloon dilatation was not performed, an external catheter was placed. Check cholangiography after 24 hours showed further expansion of the stent to 5-6mm at the level of the stenosis, equivalent to 16 - 18 Fr. drain size and free drainage of contrast (Fig. 6). The external drain was removed. After 48 hours the initial bilirubin of 500µmol/l had reduced to 297µmol/l with resolution of pruritus. The patient was discharged to a hospice and did not require any further intervention.
Colonic stent (double bare)
A 65-year-old lady with sigmoid involvement from ovarian carcinoma presented with increasing symptoms of large bowel obstruction. Endoscopic support was not available and the stricture in the proximal sigmoid colon was approached with a combination of a renal vascular sheath, catheter and guide wire. Injection of contrast showed almost complete occlusion in the apex of the junction between descending and sigmoid colon (Fig. 7). Over a stiff wire the delivery system was placed across the stenosis and a 24 x 100 double bare Egis stent deployed (Fig. 8). The stent was a little short resulting in unfavourable alignment of the proximal end in the apex of the sigmoid loop. A further stent was deployed overstenting the proximal end, in order to achieve coaxial alignment with the bowel lumen (Fig. 9).
Estimated initial stent expansion was 7mm, balloon dilatation was not performed. The patient’s symptoms resolved over 48 hours, and follow up CT showed almost complete expansion of the stents (Fig. 10). The patient remains asymptomatic after 3 months.
Covered Egis stent for gastric obstruction
A 40-year-old female patient presented with early satiety and vomiting. 2 years previously she had a laparotomy for an appendiceal carcinoma followed by cytoreductive surgery and intraperitoneal chemotherapy for omental disease 6 months later. CT showed marked eccentric thickening of the stomach from serosal disease (Fig. 11). Partial gastric obstruction was confirmed on a water-soluble contrast study (Fig. 12). Under sedation a 6 Fr. biliary manipulation catheter and a hydrophilic guidewire was passed easily into the stomach and across the stricture. Over a stiff guidewire a 24 x 100 mm double covered Egis stent was placed under fluoroscopic guidance and deployed without difficulty (Fig. 13). Within one week the patient was tolerating most foods if eaten slowly and commenced on palliative chemotherapy.
Covered Egis stent for tracheo-oesophageal fistula
A 71 year old gentleman with non-small cell cancer of the left lung and invasion of the mid oesophagus (Fig. 14) was referred for assessment of dysphagia. He had recently undergone external beam radiotherapy, and on closer questioning described coughing fits after swallowing. Water-soluble contrast swallow showed an irregular oesophagus with a fistula into the left main bronchus (Fig. 15). Due to the lack of a significant stricture the decision was made to use a large calibre straight, covered enteral stent (24 x 100 Egis double covered). The dieticians had requested nutritional support via a nasogastric feeding tube and the procedure was performed through the nose. After topical anaesthesia and conscious sedation a 6 Fr. biliary manipulation catheter was passed into the oesophagus (Fig. 16) and the fistula outlined by injection of contrast. The 10 Fr. delivery system was easily passed through the nasal passage and the stent deployed across the stricture. Injection of contrast suggested sealing of the fistula and a feeding tube was placed through the stent into the duodenum at the end of the procedure (Fig. 16e). A check swallow the following day showed the fistula to be sealed (Fig. 17). The patient had no significant dysphagia, but was continued on nutritional support for a further week before being transferred to palliative care.
















Did you know you can Register for FREE with this website?
Registration gives you full access to all of the features of WhichMedicalDevice. Find out more ...
WhichMedicalDevice is a FREE resource created by clinicians for clinicians.
Registration is free and gives you unlimited access to all of the content and features of this website.
Find out more...Registration is free and gives you unlimited access to all of the content and features of Which Medical Device. Find out more...
Which Medical Device is a community of clinicians sharing knowledge and experience of the devices and procedures we use on a daily basis. We ask that our members register with us so that we can maintain the unbiased and independent nature of our content. Registration is quick and free.
We do not make your details available to any third parties nor do we send unsolicited emails to our members. You can read our Privacy Policy here.