

Categorised under:
Interventional Radiology
>
Vascular
>
Aspiration catheters
Interventional Radiology
>
Vascular
>
Catheters
Interventional Radiology
>
Vascular
>
Thrombectomy
Interventional Radiology
>
Vascular
>
Thrombolysis
From Vascular Solutions
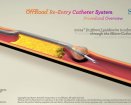
The Pronto V4 extraction catheter is designed for the removal of fresh, soft emboli and thrombi from coronary and peripheral arteries as small as 1.75mm in diameter. The uniformly large extraction lumen and embedded longitudinal wire offer maximum extraction with enhanced deliverability and kink resistance. The Pronto V4 features the patented Silva distal tip, designed to protect the vessel wall during insertion and extraction, and is currently available in 7F and 8F sizes.
The Pronto V3 extraction catheter is designed for the removal of fresh, soft emboli and thrombi from vessels in the coronary and peripheral vasculature during percutaneous interventions. Its large extraction lumen and proprietary Silva tip offer maximum extraction combined with vessel wall protection.
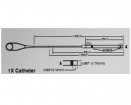
The Pronto LP is a low-profile extraction catheter designed for the removal of soft thrombus from coronary and peripheral arteries as small as 1.5mm in diameter. Compatible with any 0.014" guidewire and all 6F guide catheters (min I.D. 0.066"), it combines a very low crossing profile with a hydrophilic coating and an innovative braid- and stylet-reinforced proximal shaft.
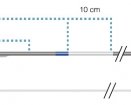
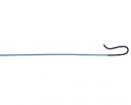
The Pronto .035" extraction catheter offers a complete system for the removal of thrombus from arteries and veins greater than 4mm in diameter. Compatible with standard 0.035" guidewires and 10F sheaths, it offers easy over-the-wire delivery. The 120-degree angled distal 4cm of the Pronto .035" provides enhanced steerability and vessel selection, and its braid-reinforced shaft increases tip control and resists kinking.
Your opinion matters to others - rate this device or add a comment






















Did you know you can Register for FREE with this website?
Registration gives you full access to all of the features of WhichMedicalDevice. Find out more ...
WhichMedicalDevice is a FREE resource created by clinicians for clinicians.
Registration is free and gives you unlimited access to all of the content and features of this website.
Find out more...Registration is free and gives you unlimited access to all of the content and features of Which Medical Device. Find out more...
Which Medical Device is a community of clinicians sharing knowledge and experience of the devices and procedures we use on a daily basis. We ask that our members register with us so that we can maintain the unbiased and independent nature of our content. Registration is quick and free.
We do not make your details available to any third parties nor do we send unsolicited emails to our members. You can read our Privacy Policy here.